

The Demographic Time Bomb: What Healthcare Can Learn from Higher Education’s Enrollment Cliff
Not too long ago, I had a conversation with a relative of mine who serves as the president of a major university. We were discussing long-range budgeting when he touched on a very important ongoing issue in their industry.
Higher education has spent years preparing for what many now call the “Enrollment Cliff.” Colleges understand that a large portion of their future applicant pool simply does not exist because many families delayed or decided against having children during the financial crisis of 2008 and 2009. At the time, the assumption was that births would rebound as the economy recovered.
They never truly did.
Nearly twenty years later, universities are now experiencing the delayed consequences of that demographic shift.
As someone who spends my career analyzing hospital reimbursement, Medicare Cost Reports, and long-term financial sustainability, I could not help but ask a similar question:
If higher education is only now feeling the effects of demographic changes that began twenty years ago, what delayed consequences are healthcare organizations only beginning to experience?
The more I researched the topic, the more one conclusion became clear. Healthcare is facing its own enrollment cliff. The difference is that universities are losing students. Healthcare is simultaneously losing future workers while gaining future patients.
A Twenty-Year Trend That Never Recovered
The Great Recession of 2008-2009 was not simply an economic event. It was a demographic turning point.
According to data from the Centers for Disease Control and Prevention, the United States had entered the financial crisis with fertility rates at or slightly above the population replacement level.
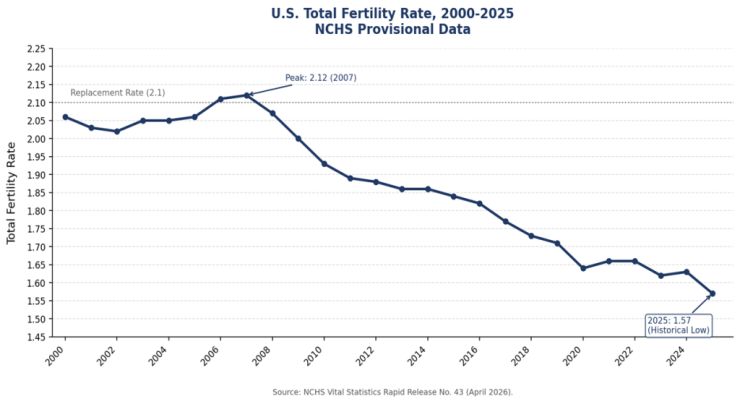
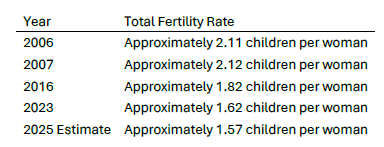
The generally accepted replacement rate necessary to maintain a stable population is approximately 2.1 children per woman. In other words, the United States has moved from replacing itself to producing roughly 23% fewer births than the replacement level would suggest.
The implications are profound.
- The children who were never born during the Great Recession are now becoming:
- The missing college applicants.
- The missing workforce entrants.
- The missing nurses.
- The missing physicians.
- The missing healthcare administrators.
- The missing taxpayers who will ultimately support Medicare.
The Great Recession may have ended, but the demographic effects never did.
The Enrollment Cliff and the Healthcare Cliff
For universities, the consequences are relatively straightforward. Fewer births ultimately mean fewer college applicants. Healthcare faces a much more complicated equation. While younger populations are shrinking, older populations are growing rapidly.
This is creating a detrimental void in the healthcare labor market as there are fewer people entering the workforce while more people are entering the years of highest healthcare utilization. Healthcare is one of the few industries where demographic change simultaneously reduces labor supply and increases customer demand.
The nursing shortage is not simply a staffing problem. It may be the leading indicator of a much larger demographic transformation.
We can also go back and look at how we got to this point. While birth rates have steadily declined, the population over age sixty-five has expanded rapidly. Twenty years ago, older Americans represented a much smaller share of the population.
Today, approximately 18% of Americans are over age sixty-five, compared to roughly 12% two decades ago, the total US population has grown by 47M people from 2004-2024 and the population of those that are 65+ has ballooned by an additional 23M Americans.
The Baby Boom generation is moving into the years associated with:
- Cardiac disease.
- Cancer treatment.
- Orthopedic procedures.
- Chronic disease management.
- Skilled nursing utilization.
- Home health services.
- Hospice care.
Healthcare demand is not disappearing.
It is aging.
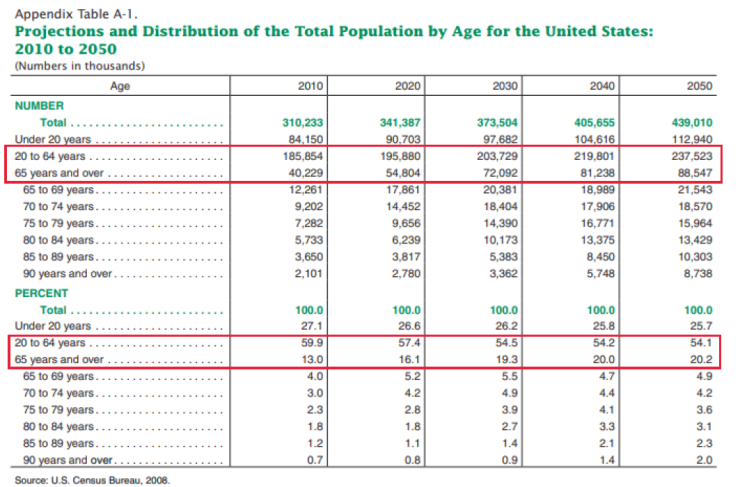
The result is a demographic squeeze. An interactive tool from the U.S. Census Bureau allows us to visualize the actual flow of aging and ripple effect of the declining replacement rate in the U.S. from 2022-2060, the striking realization is the population of those between 20-65 is set to increase from approximately 194.4M to 203.3M from 2022-2060 which is a 4.6% increase while the aging population of those that are 65+ is projected to increase from 57.6M to 88.9M which is a 54.2% increase.
The Healthcare Cliff and the growth of the 65+ population not slowing is that by the year 2040 the United States is projected to have 80M Americans that are 65+.
Based on a census projection from 2008 this issue has been in effect long before the concerns of the Covid-19 Pandemic were even a thought in the Healthcare Industry and by historical trend we are right on pace:
The Healthcare Workforce Challenge
Most discussions about healthcare labor focus on recruitment. However, the demographic challenge is larger than that. Even if nursing schools and medical schools maintain the same enrollment percentages, they will be drawing students from a smaller generation.
At the same time, many experienced clinicians will be approaching retirement.
- This presents a multitude of issues where Hospitals are entering an environment of:
- More patients requiring care.
- Fewer workers are available to provide it.
- Competition for labor intensifies.
- Wage inflation will become persistent.
What many executives have treated as a temporary labor shortage caused by the global Covid-19 pandemic may become a long-term demographic reality.
Labor and Delivery: The Canary in the Coal Mine
The recent closure of Labor and Delivery services at community hospitals, including most recently the Newark-Wayne Community Hospital decision to close their Labor & Delivery Service line, may provide an early glimpse into the future.
An excerpt from the Rochester Regional Health article:
“Consistent with declining birth rates nationwide over the last 20 years, the community Newark-Wayne Community Hospital serves has seen deliveries decline year over year, reflecting changing community needs and broader demographic trends. Combined with persistent workforce challenges, these realities have made it increasingly difficult to safely and sustainably staff a 24/7 inpatient labor and delivery unit. For Newark-Wayne OB patients who need delivery services, concentrating resources at nearby locations will enable RRH to provide a higher level of care.”
- Obstetric programs are expensive to operate and require:
- 24-hour nursing coverage.
- Obstetric physicians.
- Anesthesia support.
- Pediatric backup.
- Emergency surgical capabilities.
Those costs remain relatively fixed regardless of delivery volume. As birth rates decline, many hospitals can no longer spread those fixed costs across enough patients to maintain financial sustainability.
Labor and Delivery may be the first service line significantly affected by America’s changing demographics.
It is unlikely to be the last.
The Reimbursement Consequences
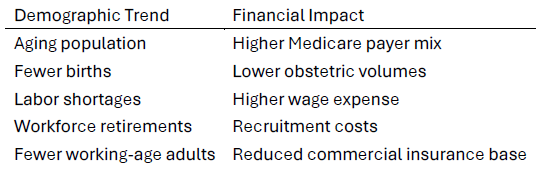
This demographic shift creates significant reimbursement challenges. Historically, hospitals benefited from a balanced payer mix that included growing commercially insured populations. However, as communities age, that mix changes.
Hospitals increasingly experience:
- Higher Medicare utilization.
- Lower percentages of commercially insured patients.
- Greater dependence on government reimbursement.
- Rising labor costs.
- Declining birth-related volumes.
These trends create what may best be described as aDemographic Margin Squeeze.
Healthcare reimbursement professionals are already seeing these trends reflected in Medicare Cost Reports through:
- Rising cost per adjusted discharge.
- Increasing labor cost allocations.
- Greater importance of Medicare DSH optimization.
- Volume Decrease Adjustment opportunities.
- Wage Index strategy.
- Supplemental payment dependency.
In many respects, reimbursement strategy is becoming demographic strategy because the populations a hospital serves will increasingly determine the payer mix, service line demand, workforce availability, and ultimately its financial sustainability.
Tomorrow’s Winners and Losers
Healthcare demand will not disappear, it will simply move.
Service Lines Facing Long-Term Pressure
- Labor and Delivery – Declining birth rates may continue to reduce delivery volumes, making it more difficult for lower-volume hospitals to support the fixed costs of obstetric programs.
- Neonatal Services – Fewer births may reduce demand for neonatal care and NICU capacity in many markets.
- Pediatrics – Smaller younger populations could soften demand for certain pediatric services, particularly in communities with declining school-age populations.
- School-Based Health Programs – Enrollment declines may reduce the need for school-centered healthcare initiatives in some regions.
- Certain Rural Family Practice Models – Rural providers serving younger and declining populations may face increasing challenges maintaining patient volumes and financial sustainability.
Service Lines Positioned for Growth
- Geriatrics – An aging population will likely drive increased demand for specialized care focused on older adults.
- Cardiology – Cardiovascular disease prevalence increases with age, supporting long-term growth in cardiac services.
- Oncology – Cancer incidence rises significantly among older populations, increasing demand for oncology care.
- Orthopedics – Aging patients often require more joint replacements, fracture care, and mobility-related procedures.
- Home Health – More patients are expected to seek treatment and recovery in their homes rather than institutional settings.
- Hospice – End-of-life care needs are likely to expand as the elderly population grows.
- Skilled Nursing – Long-term and post-acute care services may experience sustained demand from older patient populations.
- Rehabilitation – Recovery services for stroke, orthopedic procedures, and chronic conditions are expected to grow alongside population aging.
- Chronic Disease Management – As conditions such as diabetes, heart disease, COPD, and kidney disease become more prevalent, proactive management programs may become increasingly important.
Hospitals that align their strategic planning with demographic reality may have a significant competitive advantage over the next twenty years.
What Hospitals Can Do
Demographics cannot be changed, but preparation can. Healthcare organizations should begin treating these trends as structural rather than temporary.
That means hospitals should be building workforce plans ten to twenty years into the future. That it would be advantageous and proactive to use demographic forecasting alongside financial forecasting and continue to evaluate service line sustainability and margin optimization.
Hospitals will also need to continue to prioritize employee retention, expand home-based care models, and optimize reimbursement opportunities through proactive Medicare Cost Report analysis.
The organizations that thrive may not be those that react fastest to annual changes.
They may be those that recognize twenty-year demographic trends before their competitors.
Looking Back to See Forward
The most important lesson from higher education is that demographic change arrives slowly and then all at once. A decision made by millions of families during the financial crisis nearly twenty years ago is now reshaping universities across the country.
Healthcare leaders should ask themselves a similar question.
What demographic changes that began twenty years ago are only now beginning to reshape hospitals?
The evidence suggests the answer is already in front of us.
- The nursing shortage.
- Labor and Delivery closures.
- Growing Medicare dependency.
- Shifting service line demand.
- Persistent labor inflation.
- Hospital margin compression.
These may not be separate challenges at all. They may simply be different chapters of the same demographic story.
The demographic time bomb is not a future event. It is already changing the healthcare landscape, and the organizations that recognize it early will be the ones best positioned to adapt. What will the years of 2038-2044 look like due to the demographic decisions and trends that were created during the 2020-2026 years?
At Microscope, we believe that the next generation of healthcare strategy will require organizations to look beyond historical financial performance and begin integrating demographic forecasting into reimbursement planning, service line evaluation, and long-term operational decision-making.
The key markers and indicators in your Medicare Cost Reports and patient financial data should and needs to be an integral part of your systems future projections and planning. Through our Financial & Operational (F&O) Performance services, Microscope helps healthcare organizations transform these insights into actionable strategic initiatives that align resources, optimize performance, and prepare for the demographic realities shaping healthcare's future.It has always been an imperative part of the Healthcare Finance world, but the demographic trends set forth 20 years ago are now knocking on the front door for the Healthcare industry.
For more information, please contact:



